|
A 36 year-old man developed headaches and a change in personality over 6 weeks. |
![]()
![]()
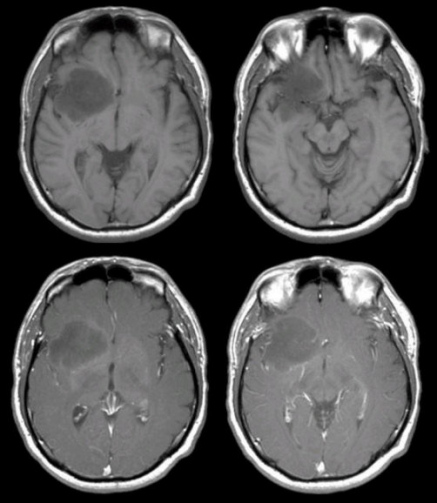
| Low Grade Glioma. (Top Row)
T1-weighted axial MRIs; (Bottom Row) T1-weighted with gadolinium
axial MRIs. Note the large low density mass in the right inferior
frontal lobe extending into the adjacent temporal lobe and basal
ganglia. There is no contrast enhancement (note the contrast in the
arteries and sinuses). This is a low grade glioma
(astrocytoma). Low-grade gliomas make up 15% of all primary intracranial brain tumors, and usually occur in young adults. They are named according to the specific type of glial cell that they derive from, and include astrocytomas, oligodendrogliomas, ependymomas, and mixed gliomas such as oligoastrocytomas that contain a mixture of different types of glial cells. Although biopsy is required to make a definitive diagnosis, the lack of contrast enhancement favors the diagnosis of a low grade glioma rather than a glioblastoma. Certain genetic conditions are predisposed to the formation of gliomas (e.g., neurofibromatosis, tuberous sclerosis). Clinical signs and symptoms depend on location. Headache and focal (or focal to generalized) seizures are common. Focal neurological deficits can occur. The World Health Organization scheme for grading gliomas from benign to progressively more malignant is as follows: ● Grade I - Pilocytic Pilocytic tumors are very benign histologically and typically occur in children. Low-grade tumors can be slow growing and controlled by surgical resection. If they recur, they are usually higher grade tumors. Anaplastic tumors are malignant tumors with mitoses and nuclear atypia. |
Revised
11/27/06.
Copyrighted 2006. David C Preston